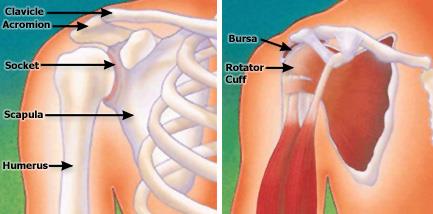
The shoulder is a ball-and-socket joint. It is made up of three bones: the upper arm bone (humerus), shoulder blade (scapula) and collarbone (clavicle).
The ball at the top end of the arm bone fits into the small socket (glenoid) of the shoulder blade to form the shoulder joint (glenohumeral joint).
The socket of the glenoid is surrounded by a soft-tissue rim (labrum).
A smooth, durable surface (articular cartilage) on the head of the arm bone, and a thin inner lining (synovium) of the joint allows the smooth motion of the shoulder joint.
The upper part of the shoulder blade (acromion) projects over the shoulder joint. One end of the collarbone is joined with the shoulder blade by the acromioclavicular (AC) joint. The other end of the collarbone is joined with the breastbone (sternum) by the sternoclavicular joint.
The joint capsule is a thin sheet of fibers that surrounds the shoulder joint. The capsule allows a wide range of motion, yet provides stability.
The rotator cuff is a group of muscles and tendons that attach your upper arm to your shoulder blade. The rotator cuff covers the shoulder joint and joint capsule.
The muscles attached to the rotator cuff enable you to lift your arm, reach overhead, and take part in activities such as throwing or swimming.
A sac-like membrane (bursa) between the rotator cuff and the shoulder blade cushions and helps lubricate the motion between these two structures.
Bursitis or tendinitis can occur with overuse from repetitive activities, such as swimming, painting, or weight lifting. These activities cause rubbing or squeezing (impingement) of the rotator cuff under the acromion and in the acromioclavicular joint. Initially, these problems are treated by modifying the activity which causes the symptoms of pain and with a rehabilitation program for the shoulder.

Partial thickness rotator cuff tears can be associated with chronic inflammation and the development of spurs on the underside of the acromion or the acromioclavicular joint.
The conservative nonsurgical treatment is modification of activity, light exercise, and, occasionally, a cortisone injection. Nonsurgical treatment is successful in a majority of cases. If it is not successful, surgery often is needed to remove the spurs on the underside of the acromion and to repair the rotator cuff.

Full-thickness rotator cuff tears are most often the result of impingement, partial thickness rotator cuff tears, heavy lifting, or falls. Nonsurgical treatment with modification of activity is successful in a majority of cases.
If pain continues, surgery may be needed to repair full- thickness rotator cuff tears. Arthroscopic techniques allow shaving of spurs, evaluation of the rotator cuff, and repair of some tears.
Both techniques require extensive rehabilitation to restore the function of the shoulder.

Instability occurs when the head of the upper arm bone is forced out of the shoulder socket. This can happen as a result of sudden injury or from overuse of the shoulder ligaments.
The two basic forms of shoulder instability are subluxations and dislocations. A subluxation is a partial or incomplete dislocation. If the shoulder is partially out of the shoulder socket, it eventually may dislocate. Even a minor injury may push the arm bone out of its socket. A dislocation is when the head of the arm bone slips out of the shoulder socket. Some patients have chronic instability. Shoulder dislocations may occur repeatedly.
Patients with repeat dislocation usually require surgery. Open surgical repair may require a short stay in the hospital. Arthroscopic surgical repair is often done on an outpatient basis. Following either procedure, extensive rehabilitation, often including physical therapy, is necessary for healing.



Osteoarthritis and rheumatoid arthritis can destroy the shoulder joint and surrounding tissue. They can also cause degeneration and tearing of the capsule or the rotator cuff. Osteoarthritis occurs when the articular surface of the joint wears thin. Rheumatoid arthritis is associated with chronic inflammation of the synovium lining which can produce chemicals that eventually destroy the inner lining of the joint, including the articular surface.


The orthopaedic evaluation of your shoulder consists of three components:
Your orthopaedic surgeon will review the results of your evaluation with you and discuss the best treatment. You and your doctor may agree that surgery is the best treatment option. He or she will explain the potential risks and complications that may occur. Dr. Craythorne may discuss donating your own blood to be used if needed during surgery.
Some surgical procedures require hospitalization for a number of days. Dr. Craythorne may discuss planning for the period after surgery. You may need to either stay in an extended care facility or have someone help you when you return home.
You may be given the option to have an arthroscopic procedure or an open surgical procedure.

Arthroscopy allows the orthopaedic surgeon to insert a pencil-thin device with a small lens and lighting system into tiny incisions to look inside the joint. The images inside the joint are relayed to a TV monitor, allowing the doctor to make a diagnosis. Other surgical instruments can be inserted to make repairs, based on what is with the arthroscope. Arthroscopy often can be done on an outpatient basis. According to the American Orthopaedic Society for Sports Medicine, more than 1.4 million shoulder arthroscopies are performed worldwide each year.

Open surgery may be necessary and, in some cases, may be associated with better results than arthroscopy. Open surgery often can be done through small incisions of just a few inches.
Recovery and rehabilitation is related to the type of surgery performed inside the shoulder, rather than whether there was an arthroscopic or open surgical procedure.
There are always some risks with any surgery, even arthroscopic procedures. These include possible infection, and damage to surrounding nerves and blood vessels. However, modern surgical techniques and close monitoring have significantly minimized the occurrence of these problems.
After surgery, some pain, tenderness, and stiffness are normal. You should be alert for certain signs and symptoms that may suggest the development of complications.
It is important that you continue a shoulder exercise program with daily stretching and strengthening. In general, patients who faithfully comply with the therapies and exercises prescribed by their orthopaedic surgeon and physical therapist will have the best medical outcome after surgery.
Your orthopaedic surgeon is a medical doctor with extensive training in the diagnosis and nonsurgical and surgical treatment of the musculoskeletal system, including bones, joints, ligaments, tendons, muscles, and nerves.
Tampa Bay Orthopaedics, Sports Medicine Specialists
Privacy Policy
Copyright 2020 @ SRL Group. All rights reserved.